

Nonblanchable Erythema
Partial Thickness Skin Loss
Full Thickness Skin Loss
Full Thickness Tissue Loss
Depth Unknown
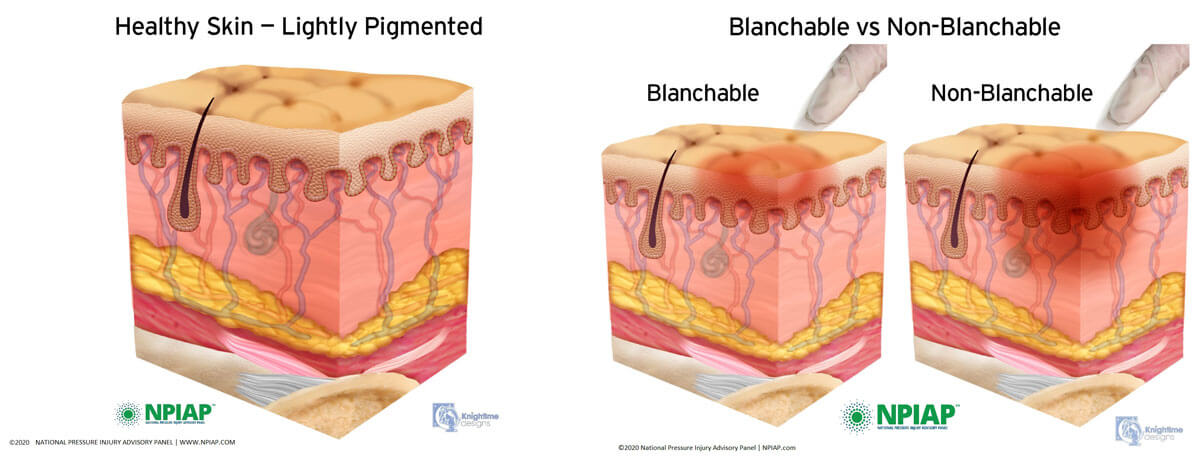
Nonblanchable Erythema
Category/Stage I : Nonblanchable Erythema
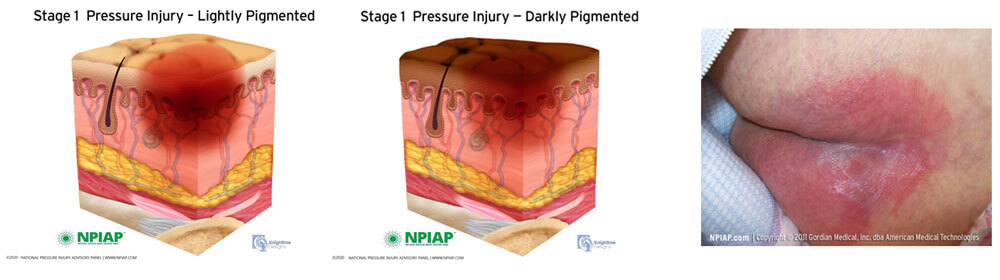
Category/ Stage I pressure ulcer/injury on the buttocks
Description
Intact skin with non-blanchable redness of a localised area usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its colour may differ from the surrounding area. The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue. Category/Stage I may be difficult to detect in individuals with dark skin tones.Partial Thickness Skin Loss
Category/ Stage II Partial Thickness Skin Loss
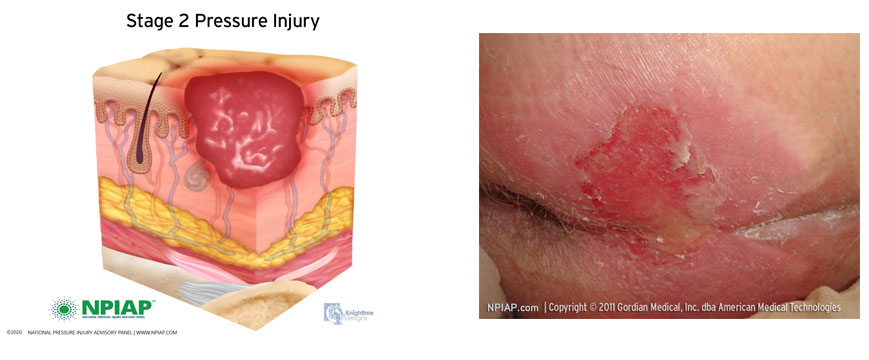
Category/ Stage II pressure ulcer/injury on the buttocks
Description
Partial thickness skin loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May present as an intact or open/ruptured serum-filled blister.
Presents as a shiny or dry shallow ulcer without slough or bruising.
Full Thickness Skin Loss
Category/ Stage III : Full Thickness Skin Loss
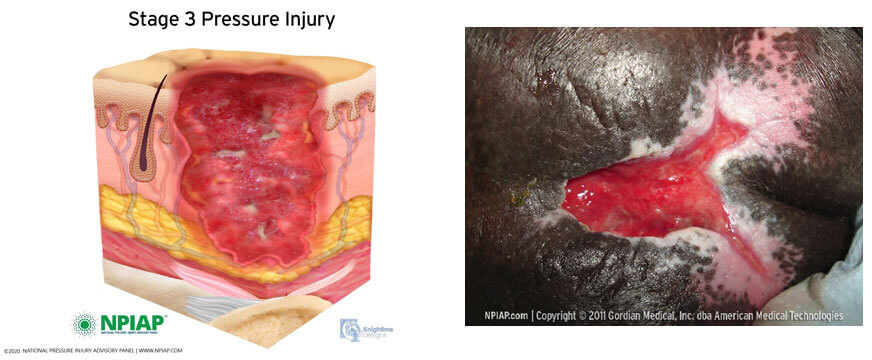
Category/Stage III pressure ulcer/injury sacrococcygeal
Description
Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon and muscle are not exposed. Slough may be present but does not obscure the depth the depth of tissue loss. May include undermining and tunnelling.
Full Thickness Tissue Loss
Category/ Stage IV: Full Thickness Tissue Loss
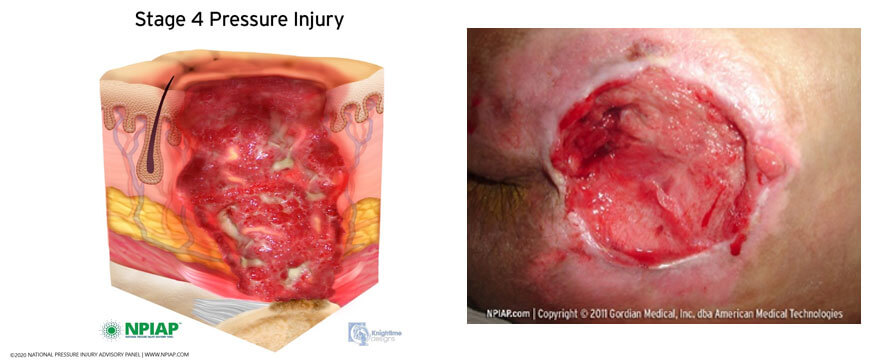
Category/Stage IV pressure ulcer/injury sacrococcygeal
Description
Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often include undermining and tunnelling.
Depth Unknown
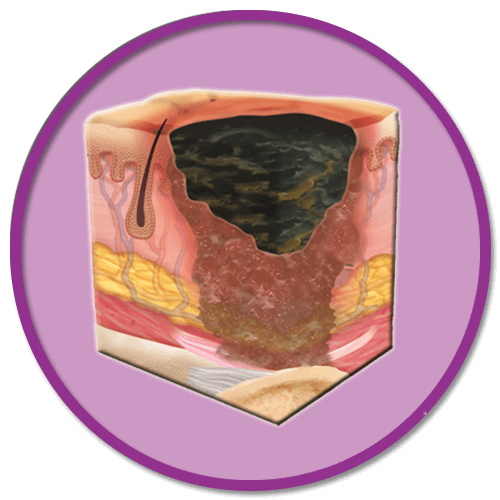
Unstageable: Depth Unknown
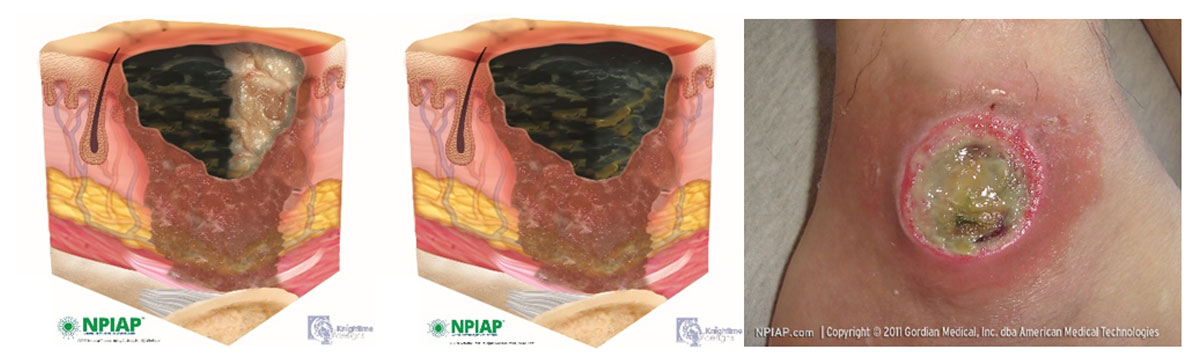
Unstageable: ankle
Description
Full thickness tissue loss in which the base of the ulcer is covered by slough ( yellow, tan, grey, green or brown) and/or eschar ( tan, brown or black) in the wound bed.
Until enough slough and/or eschar is removed to expose the base of the wound, the true depth, and therefore Category/Stage, cannot be determined.
Suspected Deep Tissue injury: Depth Unknown
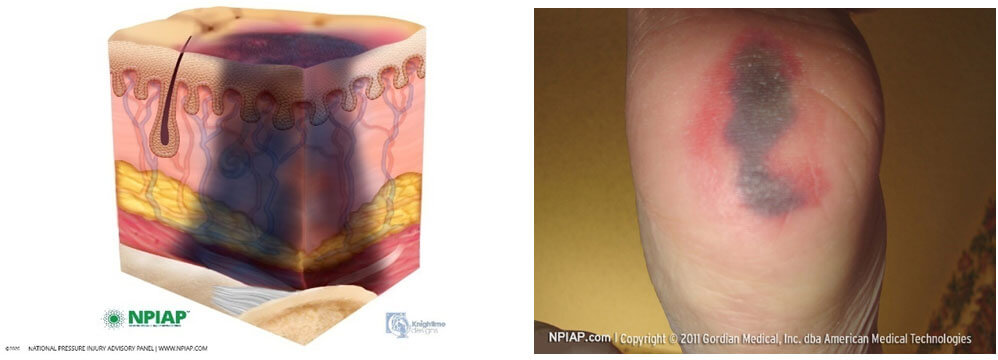
Suspected Deep Tissue Injury: heel
Description
Purple or maroon localised area of discoloured intact skin or blood- filled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue. Deep tissue injury may be difficult in individuals with dark skin tones
These are mechanical forces which cause pressure ulcer/ injuries due to one or as a combination of mechanical forces.
Pressure
![]()
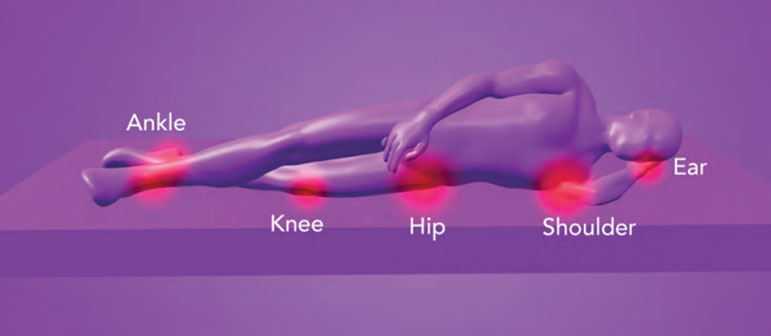
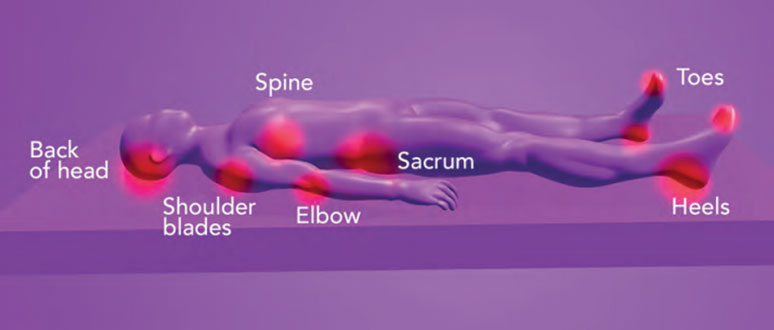
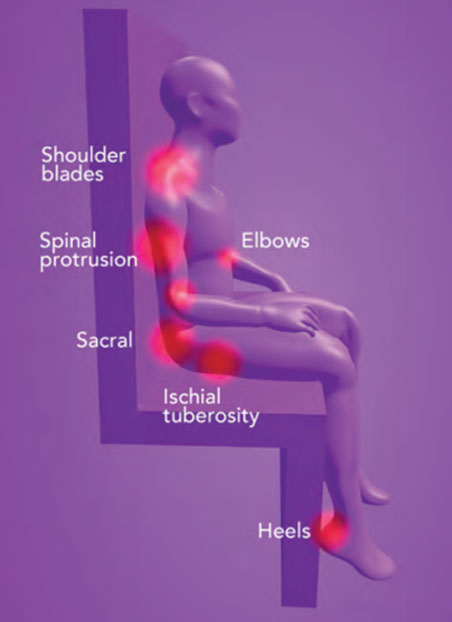
Pressure is a perpendicular force considered to be the main contributing factor to pressure ulcer/injury development. As a result of pressure generated between the body and the support surface supporting it resulting in pressure sufficient to impair blood supply, essential for healthy skin pressure ulcers/ injuries can occur. Pressure is greatest where the skin and soft tissues are compressed between bony prominences and the surface the patient is lying on. Pressure is exerted on the tissues from the downforce of the bone and underlying tissues and the upward force of the supportsurface.
Shear
![]()
Shear is a force which runs parallel to the tissues. It typically occurs when patients slide down beds or chairs due to gravity. Gravitypulls the body down, the skeleton slides down over the surface taking with it the tissue attached to the bone. The skin remains resistant and remains intact with the surface. This action results in distortion and collapse of the capillaries resulting in ischaemia, a reduction in oxygen and nutrients to the skin and potential tissue damage.
The mechanical force of pressure is also always present with shear, a combination of the two can result in greater damage to the skin.
Maturation/Moisture
![]()
When the skin is exposed to moisture which could be due to a high temperature, sweating and incontinencethis could lead to maceration of the skin over time.
Skin damage can occur due to maceration alone and can be diagnosed as a moisture lesion.
Immobility
– The main contributing factor to pressure ulcer/ injury development. The patient is unable to move in response to pain and pressure sensations.
Pain
– Patients in pain can be less reluctant or afraid to move and therefore do not relieve the mechanical forces.
Poor nutrition and hydration
– Without adequate calories, proteins, vitamins, minerals, and hydration this will impact on wound healing.
Neurological Status
– Some diseases cause loss of sensation making them aware of discomfort and the need to reposition themselves.
Body Type
– Being underweight and overweight have their challenges when addressing being at risk of pressure ulcer/injury development. Plus size patients may have difficulty in mobilising and create difficulty for caregivers sometimes resulting in poor moving and handling techniques. Patients who are underweight have less protection with a lack of cushioning over vulnerable areas.
Chronic illness
– The patient with a chronic illness can be at increased risk such as a diabetic who may have a compromised peripheral circulation and lack of sensation.
Medication
– Some medications may have an impact on the patient and their risk of skin breakdown, steroids influence the inflammatory phase of wound healing and give the skin a vulnerable papery thin texture. Strong analgesia may dull the patients senses to change position.
There are other factors which will contribute to pressure ulcers/ injuries which include:
- – Poor fitting clothing and footwear
- – Poor lifting and handling techniques
- – Inappropriate use of equipment